This article is based on research provided by North Carolina State University, School of Engineering. It was initially published in a well-respected engineering journal.1 An article on how these engineering principles could be applied to therapeutic treatment was published in September 2014.2 For further information regarding this material and for clarity, the reader is referred to that article as well as the original engineering article.
The first important point is that compression applied to the external surface of the lower limb works and provides increased venous return. This is well exemplified in many articles, including that written by Partsch in which he demonstrates that using only 6 mmHg to apply pressure to the mid-thigh not only reduces the cross-sectional diameter of both the deep femoral vein and great saphenous veins, but also results in the cross-sectional area of the thigh changing its shape from an ellipse to a much more rounded and normal contour.3
There are two basic laws of physics that explain this phenomenon. The first, “Pascal’s Law,” states that external pressure applied to the limb, such as that through an elastic device (compressive hosiery or wraps), produces internal limb pressure that is transmitted equally in all directions. This internal pressure directly decreases girth of engorged veins, which directly results in an increase in proximal venous outflow.
The second is Laplace’s law (P = T x R). A full description of the physics behind this principle is described in the Journal of Wound Care article.2 For brevity, the essential point relative to this discussion is that once tension (T) is applied to a limb with a wrap, hosiery or similar compressive device, the only way interface pressure (P) can increase is if the radius (R) increases. This law applies to any compressive device that fits around the body part (i.e. the upper or lower extremity).
The dynamics of the physical properties of compression are described and best understood using engineering laws and properties. For example, the engendering term “creep” refers to the deformation of a material over period of time due to an applied stress. An example would be an elastic material that is stretched to a set force; this material would slowly lose some of the tension force. Medical literature describes this phenomenon as material “fatigue.” However, the term “fatigue” in engineering terms refers to failure of a material when the compressive force is no longer applied. The engendering terms “fatigue” and “creep” describe two different processes, resulting with confusion between bench science and that of medicine. This article will use the appropriate engineering terms in describing the dynamics of compression.
In addition, many past articles have used the term, “sub-bandage pressure” to describe the amount of pressure (mmhg) applied to the skin under compressive wraps. Interface pressure should not be described differently for wraps and hosiery. For purposes of this article, the term “interface pressure” will reference the pressure under any type of compressive device. The author is a firm believer that better communication and understanding will occur when medicine and science use the same language and the same terms.
With a better understanding of the engineering principals of compression, the medical community can make better decisions as to how compression works to improve patient care.
Data from North Carolina State University, School of Engineering
One of the issues NCSU covered in their research was that the pressure measuring probes used to describe compression for a large number of clinical compression articles (Picopress and Kikuhime) were not accurate. These findings correlate with an article published by Thomas 2014.4 Furthermore, he concludes that the measuring devices have an error that is neither constant nor linear (proportional to the degree of pressure applied).
These findings call into question the validity of a significant amount of research in the field of compression therapy. NCSU therefore developed a new pressure measuring device using engineering fundamentals. The device is called CRIM and stands for “Center for Robotics and Intelligent Medicine” (CRIM), the division in the NCSU School of Engineering through which the data reported herein was ascertained.
In Figure 1, the three lower curves represent the creep found in three multilayer wraps that are popular in the US marketplace. The curve on the top line represents a new product indicating consistent compression throughout the five-hour session.
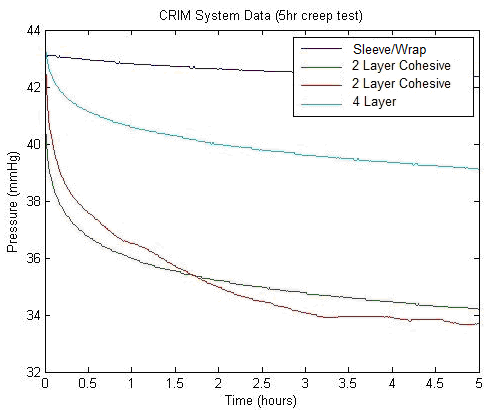
Figure 1: Creep curves. The three lower curves are 3 multilayer wraps popular in USA and indicate as much as a 25% loss of compression in only 5 hours.
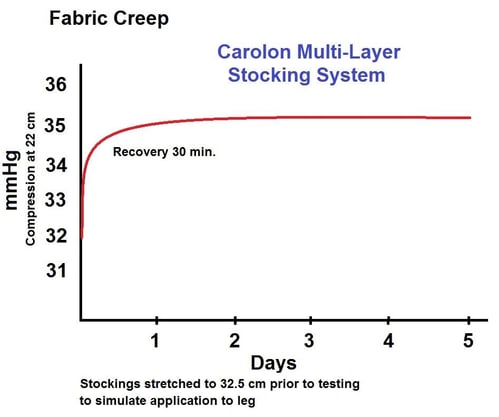
Figure 2: Creep curve of a multilayer hosiery system shows no loss of compression in 5 days
Figures 1 and 2 address one of the questions as to why some popular multilayer compression wraps that are used for a large number of patients with venous ulcers and related edema have an inherent loss of compression after application while hosiery does not. This loss of compression is due to the “creep” of the fabric—independent of a change of circumference—which may occur with a reduction of edema. When the creep of the fabric is added to the loss of circumference, a significant loss of compression will occur.
The findings demonstrated how creep impacts a large number of patients treated around the globe for venous ulcers and related edema. As an example, it is not uncommon for multilayer wraps after several days of wear to slide down the leg to the mid-calf. This can cause skin irritation and can lead to new ulcers developing along the tibial crest and other areas of the mid-calf. It has often been thought that this occurs due to loss of edema or possibly inappropriate application of the wrap. The information described in figure 1, however, describes a significant loss of compression due to creep. Combined with the loss of circumference and the variability of application of wrap systems, the resulting compressive device could lead to a significant loss of compression, allowing the compression device to more easily slide to the mid-calf and cause a reduction of the therapeutic value of the compression therapy.
What is causing a number of wraps to lose compression? Designing stable and effective fabrics for compression is a complex combination of yarns and knit structures. The applied compression and creep factor is related to these combinations, such as the size and type of spandex (primary stretch yarn) and the knit structure. Figure 1 illustrates this performance with three of the most popular multilayer wrap systems.
With regards to the application of wraps and hosiery, hosiery can have a definite advantage over wraps when it comes to a more accurate application of compression. Hosiery is designed to apply a known amount of compression within a defined circumference range. For example, a 20-30 mmHg stocking will produce an interface compression of no less than 20 mmHg at the smallest ankle circumference and no more than 30 mmHg at the largest ankle circumference as defined by a fitting chart. The compression level is not dependent on the application by the user, and the fabric can be more stable. It should be noted that if a stocking is tested on a testing device producing 25 mmHg at a defined circumference, multilayer wraps can also be applied producing 25 mmHg at the same circumference. The interface compression is the same.
A significant amount of literature suggests that two-layer wraps in general do not show consistent findings that they increase wound healing. Four-layer wraps have some ability to increase, while multilayer hosiery has shown most consistent reliability to increase wound healing. Dolibog et al., in 2014 showed similar findings in that two-layer wraps have a very poor reliability to improve wound healing.4 This study of 147 patients with unilateral leg ulcers—looking at percentage change in wound surface area or completely healed—demonstrated the following:
- Intermittent pneumatic comp tx: 57.14%
- Ulcer Stocking System: 56.66%
- Multi-layer short stretch bandages: 58.62%
- Two-Layer short stretch bandages: 16.66%
- Unna Boots: 20%
In researching these reporting findings, the authors point out the following:
- Multilayer wraps inherently have inconsistency as to how they are applied. One provider may apply a multilayer wrap with very different compression levels than another provider. Additionally, the more layers involved in the compression system, the more variables there are in how it is applied. Hosiery, on the other hand, is consistent from one provider to the next.
- Multilayer wrap systems, especially those with three or four layers, have the potential to produce high amounts of compression during application and as such require a significant level of training and experience. Each layer of compression is additive. Additionally, multilayer wraps are applied most often with the 50% overlap technique. Therefore, if the therapeutic goal is to provide 40 mmHg at the level of the ankle, one will apply the elastic wrap with 20 mmHg. Because of the 50% overlap, this would produce a therapeutic result of 40 mmHg. However, when one uses two, three or four layers of compression, one must keep in mind that each layer is additive. Using the hypothetical 20 mmHg with each layer of wrap applied a two-layer system would produce 80 mmHg, a three-layer system with 50% overlap application technique 120 mmHg and four-layer wrap as much as 160 mmHg. The provider applying the wrap must be aware of the additive effect of each layer applied and adjust the compression levels appropriately.
- The data from North Carolina State University also suggests that the fabrics they examined demonstrated a high degree of varying elasticity. This is often referred to as “stiffness."
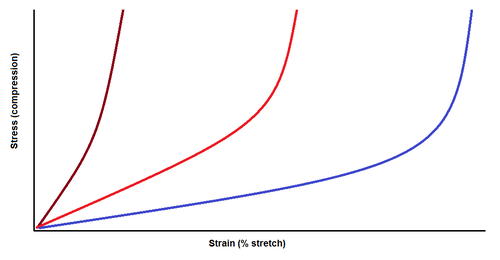
Figure 3 (above) is an example that demonstrates the stress-strain curve of a stiff, short stretch fabric such as an Unna Boot versus a long stretch fabric such as a long stretch or hosiery type of fabric. It also shows stress/strain curves that are between neither short nor long. Most of the multilayer wrap systems have a stress-strain curve the lies approximately midway between these two curves.
Because the interface compression is dependent not only on creep but highly dependent on the change in circumference, short stretch systems can increase compression quickly if the circumference increases and lose compression quickly if there is a loss of circumference. This may explain why short stretch systems such as Unna boots demonstrated very poor findings with improved wound healing, while hosiery consistently has a high correlation with increasing wound healing. The broad flattened stress/strain curve of hosiery demonstrates its ability to accommodate a range of limb circumference, correlating increasing and decreasing amounts of edema, while still maintaining therapeutic compression.
Summary of problems with multilayer wrap systems from university-based findings and other reported studies
- Multilayer wraps often cause excoriation and other irritation of skin that can lead to skin abrasions and other injuries. It is due to the overlapping of the wraps and the pressure applied to skin and interface where layers of wrap material overlap each other. This is due to the fact that most often the wraps are applied with the 50% overlap technique.
- Some self-adhesive multilayer wraps can have a high degree of “creep;” meaning, that they do not maintain the compressive force after application to the limb. Research shows that these wraps lose anywhere from 10% to 25% of their compression in as little as five hours as a result of the acquired deformation: “creep.”
- Multilayer wraps inherently have a tendency to lose the appropriate position on the limb and slide down distally from just below the knee to the mid-calf. This is a known risk factor for development of secondary ulcerations at the level of the mid-calf due to the friction and potential tourniquet effect.
- Multilayer wraps have a tendency to form creases, or “dog-ear,” most commonly around the posterior and planter aspects of the heel and the anterior ankle. This may result in the necessity to trim excess material and/or develop pressure points to the skin, leading to irritation.
- Self-adhesive multilayer wraps are occlusive and do not allow skin respiration.
- Some two-layer multilayer wraps have been shown in a significant amount of literature to have no correlation with increased wound healing.
- Four-layer wraps result in eight layers of material, increasing the “stiffness” of the overall system. As a result, the compression system becomes rigid; it is not able to expand with increased edema or reduce circumference with decreasing edema. This can result in dramatic changes in interface pressure, with only moderate or small amount changes in the amount of edema.
- Multilayer wraps have inherent inconsistency in the method in which they are clinically applied. This variable increases with the number of layers of wrapping material used in any multilayer compression system. Providers applying each layer may do so differently from one provider to the next or the same provider from day to day.
Development of a new product to address the above findings
Taking the above findings and clinical observations into account, Carolon put their research and development team to task by proposing a new treatment regimen and then, from that, working with engineering to provide a product that could be cost-competitive and address the items above. In essence, the task was to use this new data to develop a better treatment tool. The answer was to utilize the benefits of hosiery and limit the fabric limitations and the human element of variability in the application of current wrap system. This led to the development of something totally new, which is a “sleeve wrap” multilayer compression system that increases application consistency and addresses the above items one through eight.
- Skin excoriation and irritation is avoided or at least significantly reduced through the underlying sleeve, which is the first layer in this system and is in direct skin contact. The undersurface is made of terry cloth and the outside is a smooth fabric. It serves to act as a very good layer of padding to protect the skin against the overlapping interfaces of the elastic wrap.
- Creep is prevented. The outer layer that is the elastic wrap material and the main driver of compression in the system, has a fabric design that is specifically engineered to prevent (or decrease) creep as much as possible while still enhancing comfortability through its stretch characteristics, ability to maintain skin respiration, etc.
- A tendency to slide down the leg from the knee to the mid-calf is prevented or greatly reduced due to the underlying sleeve incorporating “vertical stitching.” This is a technique utilized in high quality hosiery. While it allows the garment to stretch significantly in width to adapt to increasing and decreasing levels of edema, it does not allow significant increase in stretching from distal to proximal. Therefore, it is not able to collapse on itself, which prevents or greatly resists the tendency for a multilayer sleeve wrap to slide down the leg.
- Fabric creases around the posterior and plantar heal, anterior ankle and elsewhere are prevented and/or significantly reduced through the fabric design in the sleeve and wrap. There is an appropriate amount of elasticity in all directions and the reciprocating heel in the sleeve allow both layers to conform nicely around areas of prominence in changes in shape and surface contour.
- Both the sleeve and the wrap layers allow skin respiration, are not occlusive and, most importantly, are new to the rest of the market. This is the only system that is designed to wick fluid and decrease wound maceration. The sleeve will wick fluid from the saturated dressing overlying a draining wound, and the wrap is designed to wick fluid from the underlying sleeve to the external surface of the system, allowing for evaporation or possible transfer to an absorbent dressing applied to the outside of the wrap system to absorb excessive fluid.
- There are a number of reasons why two-layer wraps have shown lack of consistency regarding enhancing wound healing. One of these may be the stress-strain curve of compression system. Compression hosiery has consistently shown a correlation with increased wound healing and has a very different stress-strain curve than the Unna boot and other multilayer wrap systems. The sleeve wrap system, when applied, provides the stress-strain curve and matches that of hosiery. This allows for a wide range of applying compression, so that the system can expand with increased edema and contract to adjust to decreased circumference with decreasing edema.
- The problem of system rigidity found with three- and four- layer wraps due to the friction between each of the layers, is nonexistent with the sleeve wrap system.
- Consistency in the application of the sleeve wrap compared to other multilayer wraps is due to the fact that the sleeve application is consistent from provider to provider and from day to day with the same provider. A variable application technique is tremendously reduced due to the fact that there is only one layer of wrap that is dependent upon the individual method of application. Two- three- and four- layer wraps have increasing variability with each layer of wrap applied.
- The underlying sleeve contains copper ion; it will not wash out with multiple washings. Copper has been demonstrated in literature to be antimicrobial to multiple bacteria, fungi, yeast, bed mites, HIV, influenza, VRE, MRSA, etc.
- The sleeve wrap is reusable. When applied, if it is uncomfortable, it can be easily adjusted. If not soiled upon dressing change, it can be reapplied at the same office visit. If soiled, it can be washed and dried in a washer machine and dryer, and has been field-tested for 10 washings/machine dryings without any loss of compression.




Concluding remarks
This article discusses how research—that was performed first independently—led to an analysis of methods to address and correct problems identified, as well as ultimate development of a new treatment regimen and a new product to improve patient care in a cost-competitive manner.
The research performed at North Carolina State University demonstrates conclusive data indicating that multilayer wraps used for compression therapy have significant “creep.” Other problems with currently utilized therapy for venous ulcers and related edema from other studies is also cited in this article. These inquiries were initiated by Carolon, a company historically involved in compression therapy. Members of the Carolon R&D team had questions about inconsistencies in past literature and scientific studies regarding compression therapy relative to patient care. The intent was to clarify these issues based on engineering principles and laws of physics. This then led to a new treatment regimen and new product development addressing each of the problems identified in current therapies. The “sleeve wrap” combines the benefits from hosiery with a totally newly designed sleeve and new elastic wrap material while removing many of the negative aspects of the current multilayer wraps available.
Steven Kravitz, DPM, FAPWHc, FACFAS is Medical Director, of Carolon; Assistant Professor, Temple University School of Podiatric Medicine; and Executive Director of the Academy of Physicians in Wound Healing (APWH)
For more information on the Carolon Sleeve Wrap, contact Carolon at [email protected], or by phone at 800-334-0414. For international calls dial 336-969-6001.
References
1. Hegarty-Carver, M., Kwon, C., Oxenhamb, W., et. al. Towards Characterizing the Pressure Profiles of Medical Compression Hosiery: an Investigation of Current Techniques, The Journal of the Textile Institute. 2014. July 30:1-10 online publication
2. Hegarty-Carver, M., Grant, E., Kravitz, S. Research into Compression Fabrics Used in Compression Therapy and
Assessment of their Impact on Treatment Regimens, Journal of Wound Care, Academy of Physicians in Wound Healing Supplement. 2014. 23: S14-S22
3. Thigh Compression. H Partsch, G Mosti Phlebology 2008:23:252-258
4. Practical limitations of two devices used for measurement of sub-bandage pressure: Implications for clinical practice; S. Thomas, Jour Wound Care, vol 23;NO 6; June 2016
