by David Wright, MD, Ariel Soffer, FACS, RCS MD, FACC, Shayna Soffer, Tanya Ramadoss, BBA
Screening for Chronic Venous Insufficiency with Point of Care Thermography
With the global venous and lymphatic community planning to meet in Miami at the joint UIP/AVLS conference in 2023, we would like to highlight some of the emerging data on improved methods for screening for common diseases seen by these circulatory experts.
Recently, Eberhard Rabe from Germany along with his French colleague conducted an international survey using a representative sample of the general population from eight countries.1 They found that the prevalence of self-reported signs and symptoms of chronic venous insufficiency (CVI), the most common form of venous or lymphatic disease, is about 22.0%.
This large study showed most individuals with CVI symptoms do not seek help from a physician, and those who do tend to have more severe diseases that could have been detected and treated earlier. The results of this study reinforce the need for greater international awareness of CVI and better screening techniques to ensure timely diagnosis and appropriate treatment.
CVI is a worldwide problem, with patients across the globe having similar symptoms. Irrespective of which country is surveyed, around 2-3% of those will go on and get the most dreaded and expensive manifestation, venous leg ulcers (VLUs).2 CVI is estimated to cost the world billions of dollars in lost productivity and healthcare costs. Thus, many countries have begun to look at earlier and better ways of screening for CVI in the hopes of reducing the impact on their populations and healthcare systems.
Throughout the world, screening for CVI is similar in nature. A thorough history and physical exam looking for signs of venous insufficiency with symptoms like leg swelling or discomfort and signs like varicose veins and characteristic skin changes are commonplace. When suspicion of CVI exists, several tests that often give clues to the source of venous hypertension can be performed in the outpatient setting during the initial evaluation. The cough impulse test (performed by palpating the thigh at the fossa ovalis over the saphenofemoral junction), the Brodie-Trendelenburg test, and a few others have been used to screen for CVI, but most clinicians rarely utilize these types of tests due to their lower sensitivity and specificity (compared to duplex ultrasound) and practical concerns, such as patient positioning.
Thus, the most common screening test for CVI in most countries today and what is considered the “gold standard” is duplex ultrasound (DUS). However, in many parts of the developing world and even certain underserved areas of more advanced countries, DUS is considered challenging to provide as a screening tool for many of the at-risk populations. These challenges seem to be mostly due to the costs, specific training, and lack of easy portability of most DUS systems.3
Additionally, the physical nature of DUS requires contact over an extended period of time, making it more of a challenge, particularly during pandemic-type conditions, as was recently experienced.
To further understand the importance of having both a widely available screening test, as well a highly correlated diagnostic test, one must understand the difference between the two tests. The main difference between a screening and a diagnostic test is the purpose of each.
Screening tests are primarily used for the early detection of disease or risk factors for disease. Diagnostic tests are used to establish the presence or absence of disease. Screening tests are often done among people with limited symptoms who may have a higher risk of developing disease. Johns Hopkins lists common screening tests that have impacted medicine to be cholesterol, Pap smears, mammography, and colonoscopy to name a few.
Ambulatory Blood Pressure (ABP) and Arterial Brachial Index (ABI) are commonly considered screening tools in assessing arterial hypertension and stenotic disease. ABP and ABI, when used as screening tools often lead to the confirmatory diagnostic test, DUS in order to establish the presence or absence of the disease itself.
Unfortunately, there is no widely agreed upon or utilized screening tool for CVI, often considered the most prevalent circulatory disease in people. However, as the clinical, economic, and psychological costs of CVI are better understood, global attention has begun to focus on earlier and more widespread detection. If one was to design an ideal screening test, we would start with a disease that has significant prevalence, and develop a low cost non-invasive, non-contact, non-radiating tool. It should have limited false negatives and very reliable positive findings when compared to the gold standard.
Point of Care Infrared Thermography (POCIT) has been identified as the potential screening tool for a disease process as ubiquitous as venous insufficiency.
Thermography All Over the World
Investigators across the globe have begun to show interest in POCIT as a bespoke screening tool for CVI. Below is a current review of some of the international data being published regarding the use of POCIT for the screening (and optimal mapping) of CVI.
The Polish Data: In 2014 and then in 2017 Cholewka et al. from Poland, described their findings for use of, what they termed, “thermovision” for detecting CVI in patients. In fact, they discuss the possibility of thermography being able to detect CVI even earlier than seen in standard DUS.4
They used a form of subtraction analysis to isolate areas of increased temperature in limbs suspected of having CVI.

Figure 1: The Polish Data
The Indian Data: With acknowledgments made to the Bangladesh Ministry of Health and Social Welfare Bangladesh, in 2021 Dr. Kelly-Hope et al., showed a fascinating series on how lymphedema is clearly seen in unilateral filariasis.5 Although this study emphasized the lymphatic system, venous screening implications are obvious as well. This unequivocal thermographic image has found use in underserved tropical environments and could change the way this devastating infection is ultimately detected.
Infrared Thermal Imaging as a Novel Non-Invasive Point-of-Care Tool to Assess Filarial Lymphoedema published by Louise A. Kelly-Hope, et al. See amazing pic below.

Figure 2: The Indian Data
The Brazilian Data: The Brazilian Thermology Society has recently met and updated many of its previous recommendations.6 They boast a two-year fellowship program and use different heat patterns across the body for a variety of disease recognition. In San Paulo, Mendonca et al.’s most recent publication showed how thermography was able to help differentiate the different etiologies of leg ulcers and possibly screen for them.7
Considering that determining whether a leg ulcer is of venous origin remains a major problem for wound care clinics all over the world (as the treatment options are so different), this development may be of enormous value in the future.
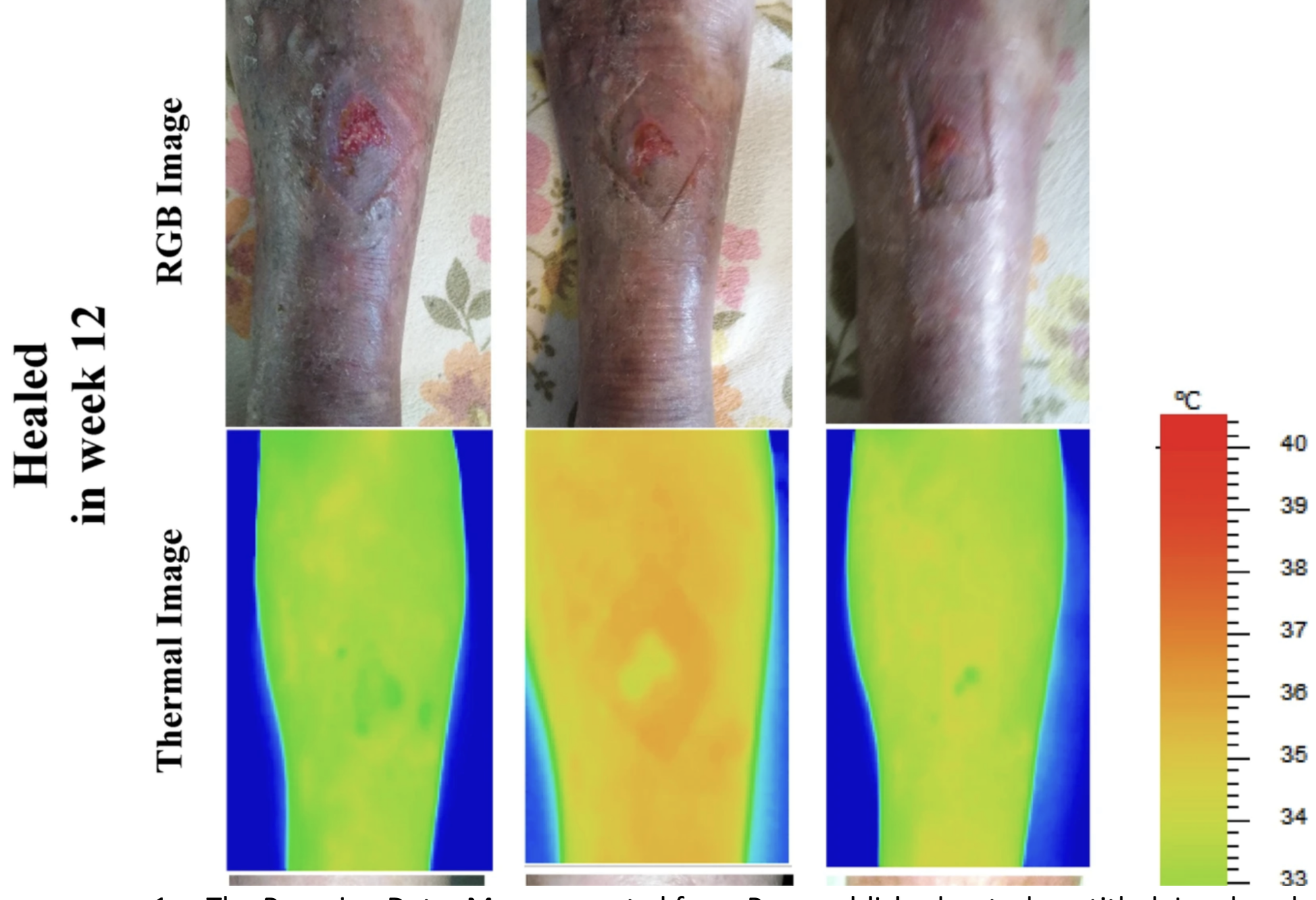
Figure 3: The Australian data
The Australian Data: An Australian research group used screening thermography to detect disease as well as to predict which venous leg ulcers might be most likely to heal.8 Dr. Rajna Ogrin, Senior Research Fellow, Bolton Clarke Research Institute said, “A non-contact method like thermal imaging would be ideal to use when managing wounds in the home setting to minimize physical contact and therefore reduce infection risk.”9
The Peruvian Data: Menenses et al. from Peru published a study entitled, “Landmark Detection of Suspicions of Varicose Veins in the Legs Using Thermal Imaging.”10 They investigated the use of POCIT and post-processing software to superimpose the thermal images with the photographic images. This helped them to maximize CVI detection which was subsequently correlated with DUS. They mention that in the future they hope to be able to predict the depth (and thus quantitative analysis) of varicose veins as well.
The Israeli Experience: An offshoot of the Israeli Defense Forces, Opgal is currently investigating POCIT in conjunction with the highly acclaimed national hospital, Sheba Medical Center, near Tel Aviv. “Thermal cameras can become as widespread in doctors’ pockets as stethoscopes,” says Sheba Medical Center Innovations Chief Prof., Eyal Zimlichman. Not only do they have an interest in screening for circulatory disorders, but they are currently investigating intraoperative use as well as ICU utility.
As many high-tech developments have come out of public, private, and military experiences, they are likely to continue to add to the world's understanding of the importance of POCIT and venous screening.

Figure 4: The Israeli experience
The American Data: Much of the data has come out of two main centers in South Florida and Louisiana, which have collaborated to publish data showing the very high sensitivity and specificity in the detection of venous insufficiency as correlated with duplex Ultrasound.11 Dr. Craig Walker said in his editorial in Vascular Disease Management, “Point of Care Thermography could become a cost-effective screening tool. This could also potentially improve the diagnostic accuracy of ultrasound by highlighting areas of interest for the technician to evaluate.”12
Currently, Nova Southeastern University in Davie, Florida, and the Levan Center of Innovation are working with USA Therm, Inc. to continue to prove the utility of POCIT for screening at-risk populations for CVI. Their emphasis is to help diagnose CVI as early and frequently as possible, allowing patients to understand the etiology of their symptoms best and begin the process of appropriate graded compression. It is anticipated that a community screening study utilizing thermography will be held simultaneous to the upcoming AVLS/UIP in Miami in 2023.
Summary
If we can properly utilize a non-invasive, non-contact, portable, and affordable screening medical device like Point of Care Thermography to detect CVI earlier, the increased awareness and earlier detection might benefit so many. The importance of earlier detection leading to earlier diagnosis with DUS may lead to multiple forms of modern intervention in this chronic and often debilitating disease progression. Our hope as part of a global medical community having meetings like the AVLS/UIP in Miami 2023, is we can share our combined experiences for the common good.
References:
- Rabe, Eberhard. Régnier, Catherine. Goron, Fabienne. Salmat, Ghislaine. Pannier, Felizitas. The prevalence, disease characteristics and treatment of chronic venous disease: an international web-based survey Journal of Comp Eff Res 2020 Dec;9(17):1205-1218. doi: 10.2217/cer-2020-0158. Epub 2020 Oct 20.
- Probst, S. Weller, C.D. Bobbink, P. Saini, C. Pugliese, M. Skinner, Monica Buehrer. Gethin, G. Prevalence and incidence of venous leg ulcers—a protocol for a systematic review. Syst Rev 10, 148 (2021). https://doi.org/10.1186/s13643-021-01697-3
- Zygmunt Joseph A. Duplex ultrasound for chronic venous insufficiency. J Invasive Cardiol. 2014 Nov;26(11):E149-55. PMID: 25364006.
- Cholewka, A. Kajewska, J. Marek, K. et al. How to use thermal imaging in venous insufficiency?. J Therm Anal Calorim 130, 1317–1326 (2017). https://doi.org/10.1007/s10973-017-6141-7
- Douglass, J. Mableson, H. Martindale, S. Jhara, ST. Karim, MJ. Rahman, MM. Kawsar, AA. Khair, A. Mahmood, AS. Rahman, AF. Chowdhury, SM. Kim, S. Betts, H. Taylor, M. Kelly-Hope, L. Effect of an Enhanced Self-Care Protocol on Lymphedema Status among People Affected by Moderate to Severe Lower-Limb Lymphedema in Bangladesh, a Cluster Randomized Controlled Trial. J Clin Med. 2020 Jul 30;9(8):2444. doi: 10.3390/jcm9082444. PMID: 32751676; PMCID: PMC7464742.
- Brioschi, Marcos. Introducing Brazilian Thermology Society, ICGMT, and PAJMT. Pan American Journal of Medical Thermology, [S.l.], v. 2, n. 2, p. 55-57, dez. 2015. ISSN 2358-4696. doi: http://dx.doi. org/10.18073/2358-4696/pajmt.v2n2p55-57.
- Mendonça AC, Jior JAF, Frade MAC, Barbosa RI, das Neves LMS, de Jesus Guirro RR, de Oliveira Guirro EC. Thermographic Characterization of Cutaneous Ulcers of Different Etiologies. J Med Syst. 2020 Aug 3;44(9):160. doi: 10.1007/s10916-020-01612-8. PMID: 32748024.
- Ogrin R, Motin MA, Aliahmad B, Elder K, Anderson J, Kumar D. Can Thermal Imaging Technique be Used to Predict the Healing Status of a Venous Leg Ulcer? Int J Low Extrem Wounds. 2023 Mar;22(1):85-92. doi: 10.1177/15347346211002351. Epub 2021 Apr 15. PMID: 33856237.
- RMIT University. "Thermal imaging offers early alert for chronic wound care: Textural analysis of thermal images of venous leg ulcers can detect if a wound needs extra care." ScienceDaily. ScienceDaily, 30 June 2021.
- Meneses-Claudio, Brian. Alvarado-Diaz, Witman. Roman-Gonzalez, Avid. “Detection of Suspicions of Varicose Veins in the Legs using Thermal Imaging” International Journal of Advanced Computer Science and Applications(IJACSA), 10(5), 2019. http://dx.doi.org/10.14569/IJACSA.2019.0100554.
- Soffer, Ariel. Caine, Marcus. Hardigan, Patrick. Gefin, Ryan. Young, Eric. Deiner, Joshua. Wright, David. Vascular Disease Management. 2021 Mar; ISSN 2152-4343
- Walker, Craig. The Potential of Thermography as a Practical Screening Tool for Superficial Venous Insufficiency. 2020 Nov, ISSN 2152-4343.
