IN JUNE 2020, the Lipedema ICD-10-CM Committee, with support from the American Vein & Lymphatic Society (AVLS), submitted an application to the US Centers for Disease Control and Prevention to establish new ICD-10-CM codes for lipedema and lipolymphedema, two related adipose tissue disorders.
Currently, these conditions can only be coded using less specific codes. If approved, the new codes would help facilitate the accurate diagnosis and treatment of patients with lipedema or lipolymphedema. They will also support research efforts, such as in the recruitment of participants for clinical trials and patient registries. These changes would also help distinguish lipedema and lipolymphedema from related but distinct diseases.
LIPEDEMA
Lipedema was first described in 1940 by physicians at the Mayo Clinic. This condition is characterized by symmetrical enlargement of loose connective tissue of the limbs. This can occur in the hips, buttocks, thighs, lower legs and arms, while generally sparing the feet, hands, and trunk.
In the early stages of lipedema, most women have a normal appearance above the waist
Symptoms of lipedema vary from person to person, but this condition is often painful. Some of the other defining characteristics of lipedema include easy bruising and continued swelling of the legs even when they are elevated or after weight loss. The increased bruising may be caused by greater fragility of the small blood vessels within the lipedema fat.
Lipedema occurs almost exclusively in women. The precise prevalence of lipedema is not known. It is estimated between 5–39 percent of post-pubertal girls are affected.1,2 Using the lower prevalence estimate, as many as nine million women in the United States could have lipedema, and the majority of them are undiagnosed.
Deposition of fatty tissue usually begins during a period of hormonal and weight change, such as puberty, pregnancy, or menopause. The fat deposits and body mass index (BMI) increase as the disease progresses. The exact cause of lipedema is unknown, but genetic causes are suspected—up to 60 percent of women with lipedema have an immediate family member who is also affected.
The diagnosis of lipedema is frequently missed because clinically, it resembles lymphedema, a condition involving an increase in the collection of lymphatic fluid in the body. Women may also be misdiagnosed as only obese, even when lipedema is present. Although some women with lipedema are overweight or obese, these are distinct conditions. However, obesity can worsen the clinical progression of lipedema. Uniquely, the lipedema fat is resistant to loss through dietary changes, exercise, or bariatric surgery. However, these treatments may help patients who have lipedema and are obese to maintain a healthy weight.
There is no cure for lipedema. Treatment is aimed at managing symptoms, especially pain, edema, and the disproportionate size of the trunk and extremities. A secondary goal of treatment is to prevent complications, including skin infection and reduced mobility due to the accumulation of lipedema fat.
The main conservative treatment is complete decongestive therapy (CDT). This involves several approaches, such as manual decongestive therapy, wrapping, compression garments and pumps, and exercise. Increased physical activity aids both in edema reduction—through the pumping action of the calf muscles—and weight loss. Likewise, dietary changes may aid patients with obesity by helping them to lose and maintain weight.
For patients who do not respond well to these conservative and supportive measures, lymph sparing liposuction using specialized techniques is the treatment of choice for certain patients. This may involve water-jet assisted liposuction or tumescent techniques. In some cases, surgical excision of the lipedema fat is the only option to improve a patient's mobility.
LIPOLYMPHEDEMA
Lipedema is sometimes misdiagnosed as lymphedema, a chronic and progressive swelling caused by a blockage in the lymphatic system. This obstruction results in an increased collection of protein-rich lymphatic fluid in the tissues, which can lead to changes in the skin, fat, muscle, and other tissues. Lymphedema is a lifelong condition with no cure. It affects an estimated 250 million people worldwide. Lymphedema swelling can occur anywhere in the body, including the arms, legs, face, neck, chest, and genitals.
It can cause a number of complications, including recurrent bouts of cellulitis, lymphangitis, bacterial and fungal infections, lymphangio-adenitis, deep vein thrombosis (DVT), severe functional impairment and the need for amputation of the affected limb. Severe cases of untreated lymphedema can result in soft tissue cancer known as a lymphangiosarcoma.
Lymphedema can be either hereditary (primary) or acquired (secondary). Secondary lymphedema is more common, affecting about one in 1,000 Americans. This can result from damage to the lymph nodes or lymph vessels due to surgery, radiation treatment for cancer, blockage by cancer cells, infection, or other factors. Primary lymphedema is rare, with only about one in 100,000 Americans affected.
Lymphedema can also occur secondary to obesity or lipedema. Lymphedema is a common comorbidity in people with a BMI greater than 50. In the United States, 42.4 percent of adults were considered obese in 2017 –2018, with 9.2 percent of adults considered severely obese, according to the US Centers for Disease Control and Prevention. Severe obesity is defined as having a BMI of 40 kg/m2 or greater. This puts a substantial fraction
of American adults at risk of lymphedema.
The co-occurrence of lipedema and lymphedema appears to be fairly common, with some studies suggesting that up to 15–17 percent of women have both conditions. However, these two conditions have several distinguishing characteristics, including the sparing of the hands and feet in lipedema. During the later stages, women can develop a type of lymphedema called lipolymphedema. This is caused by increased tissue pressure and damage to the lymphatic vessels due to the accumulation of lipedema fat.
PROPOSED ICD-10-CM CODE CHANGES
Lipedema does not currently have a unique ICD-10-CM code and can only be coded using non-specific codes. The proposed changes include adopting specific codes for the three stages of lipedema, as well as for related but distinct diseases. The changes also call for the deletion of certain less-useful codes for related conditions.
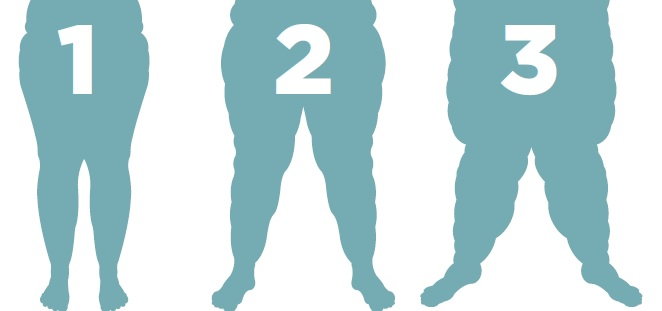
Like many diseases, lipedema tends to progress over time. The severity of this disease can be described in three stages, each with distinct characteristics. These stages are:
- Stage 1 Smooth skin with an increase in subcutaneous tissue (lipedema fat).
- Stage 2 An irregular skin surface with indentations and a nodular appearance
of the subcutaneous tissue. - Stage 3 Large growths of nodular, fat-causing lobules and severe deformity of the thighs and around the knee, both of which can inhibit mobility.
New ICD-10 codes offer a number of benefits, including improved identification, tracking, and research involving women with lipedema. This would enable physicians to better understand the prevalence of this condition, as well as support the recruitment of
patients for clinical trials and registries.
Having ICD-10-CM diagnostic codes for the three stages of lipedema would also help raise awareness of this condition among health-care providers.
The proposed ICD-10-CM changes include introducing a new code for each stage, as
well as a code for “Lipedema, not otherwise specified.” These fall under a new “lipomatosis” subcategory. Another proposed change is the addition of a new code for lipolymphedema.
Having separate codes for each stage of lipedema would facilitate studies of how/if women progress—or regress—from one stage to another. The codes would also enhance clinical assessment and care.
Another proposed change is the addition of new unique codes for Madelung's disease, Dercum's disease, and lipomatosis, not otherwise specified. These diseases are discrete conditions from lipedema.
Madelung's disease is a rare disease that results in an accumulation of fat primarily on the upper body, such as around the neck and shoulder areas. The code changes include the addition of two synonyms for Madelung's disease—multiple symmetric lipomatosis and Launois-Bensaude lipomatosis.
Dercum's disease is a rare disorder characterized by growths of multiple, painful fatty tumors (lipomas) under the skin and sometimes all over the body. The proposed changes also include eliminating the existing code for adiposis dolorosa, which is incorrectly used to describe both lipedema and Dercum's disease.
The code for “lipomatosis, not otherwise specified” would be used to describe a rare, usually autosomal, dominant condition in which multiple lipomas that are generally not painful form on the body, most often on the trunk and extremities.
The ICD-10 codes currently used in Germany have specific codes for lipedema and its three stages, as well as for Dercum’s disease. Aligning the ICD-10-CM codes used in the United States with the ones used in Germany will help facilitate joint research between the two countries.
Together these changes will enhance the care of women with lipedema or lipolymphedema well into the future.
Lipedema ICD-10-CM Committee was spearheaded by Jeffrey Restuccio CPC and included Karen Herbst Ph.D., MD, Nadiv Shapira MD, and Thomas Wright MD.
REFERENCES:
1. Reich-Schupke S, Schmeller W, Brauer WJ, Cornely ME, Faerber G, Ludwig M, Lulay G, Miller A, Rapprich S, Richter DF, Schacht V, Schrader K, Stucker M, Ure C. S1 guidelines: Lipedema. J Dtsch Dermatol Ges 2017; 15:758-767. doi: 710.1111/ddg.13036.
2. Marshall M, Schwahn-Schreiber C. Prävalenz des Lipödems bei berufstätigen Frauen in Deutschland (Lipödem-3-Studie). Phlebologie 2011; 3:127-134
